In the year 2001, I went every week to a day program for older people with a history of mental illness. It was in Washington, DC. I would typically go with the flow, sit there with the residents or participate in an activity, while trying to elicit some stories and memories of their lives. This process got encapsulated in booklets I made for each of them, before I left. More ten years later, I look back at this experience in this short piece « Life stories and the ethnographic encounter: engaging in the social experience of mental illness (pdf file) » (presented at the 2013 Society for Medical Anthropology Meeting in Tarragona, Spain).

It is 9 am. I am in the elevator of a Presbyterian Church in downtown Washington, DC. John is standing next to me. We don’t talk, but he is smiling broadly, as he often does. His smile shows the hole of his two missing front teeth. He is a skinny and energetic man in his late sixties. We often share this elevator ride, me arriving for my day at the center, John coming back from his long morning walk. I take his smile as a way of welcoming me here. But I also sense something else in our mostly silent encounters in the elevator, a much more tenuous feeling that we are both sensitive to the sweet irony of life.
When I come in the huge hall that is the center’s day room, I spot Doris and Martha in the reading corner. They seat in their big chairs, next to the magazines. I go to them and say hi. We talk a little about daily news, how was the weekend, what is for lunch. Sometimes I get bored or even depressed by the sole sight of these two, because of how predictable our exchanges are. Yet, I feel compelled to go and talk with them, to adopt their chitchatting. I guess they seem to be expecting that from me and because somehow I am here to be agreeable to them.
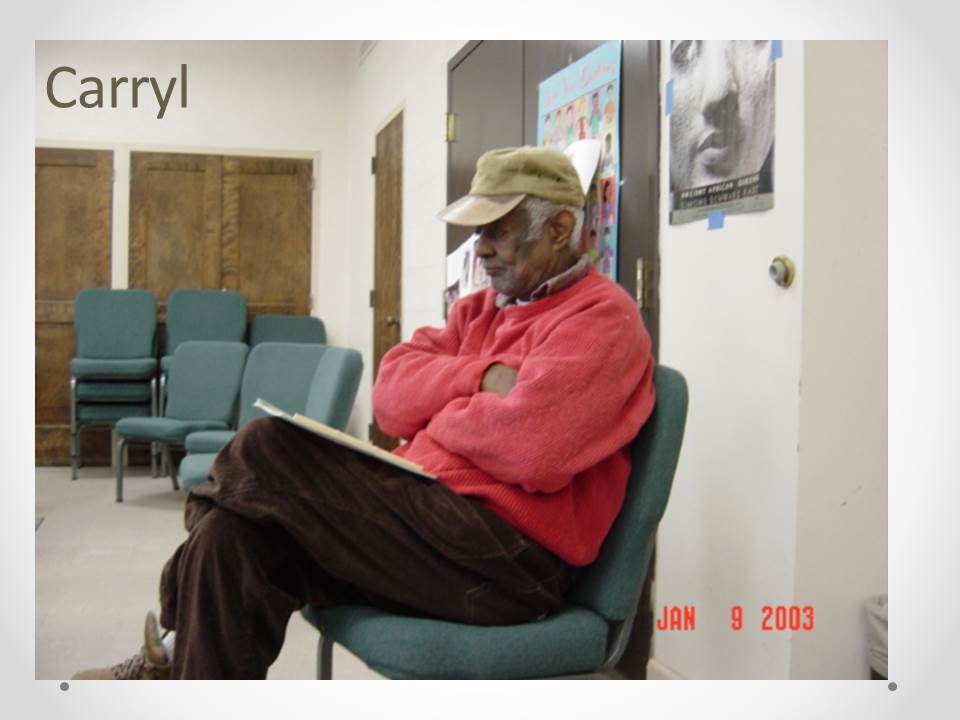
After greeting Lisa and Dan, the art therapist and the case manager, in the office room, I go and see Carryl, who is sitting motionless on a chair against the wall. 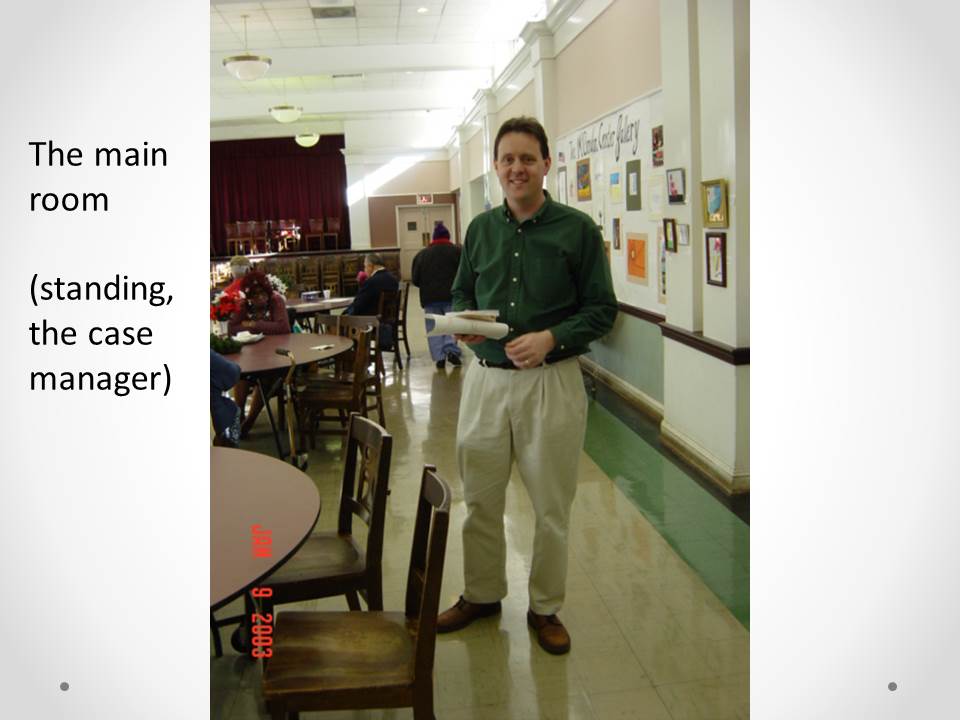 He is waiting for me in a quiet, thoughtful way. Today we are to continue the interview session from last week. Once we are seated in the small meeting room, I turn on the recorder and he starts commenting on the story that he told me last time. He says he thought it over and that maybe he could have fought more when his wife left him. We then discuss the differences in the treatment of mental illness in France and in the US. Judging from the intensity he puts into them, it looks like our moments together offer him a space and an opportunity to think that he aspires to.
He is waiting for me in a quiet, thoughtful way. Today we are to continue the interview session from last week. Once we are seated in the small meeting room, I turn on the recorder and he starts commenting on the story that he told me last time. He says he thought it over and that maybe he could have fought more when his wife left him. We then discuss the differences in the treatment of mental illness in France and in the US. Judging from the intensity he puts into them, it looks like our moments together offer him a space and an opportunity to think that he aspires to.
A little less than an hour later, we end the discussion and we join a dozen other residents and Lisa in the activity room. Today a drawing session is planned; the theme is: “drawing a life tree”. This was Lisa’s idea, which she suggested last week, when we discussed my project of working on the residents’ “life stories”.
 Yet, it is not clear to me, or to her or the others in the room, what exactly a “life tree” should be. For about an hour, everyone, including myself, tries to make something out of this fuzzy instruction in his or her own way. As usual, John ignores it altogether and starts to write in small caps on the blank page. Today, his title is about God. It very often is. I don’t know where all this is going.
Yet, it is not clear to me, or to her or the others in the room, what exactly a “life tree” should be. For about an hour, everyone, including myself, tries to make something out of this fuzzy instruction in his or her own way. As usual, John ignores it altogether and starts to write in small caps on the blank page. Today, his title is about God. It very often is. I don’t know where all this is going.
These scenes are taken from a one-year long fieldwork experience in a day treatment center for older people with a history of mental illness – and currently still in treatment. They are reconstructions of typical encounters, based on my recollections and field notes.
The three people I singularized in this introduction, John, Doris and Carryl, are all people who engaged in the “life story project” I was “co nducting” at the center. The project was quite vague initially; it took shape slowly. Retrospectively, it consisted in eliciting stories and memories from residents during group sessions, using drawings and writings (draw a life tree, your first job, your first memory…). I also collected each resident’s narrative through repeated interviews or informal discussions during the day I spent at the center weekly. This resulted in individual booklets I made for each resident. These booklets contained pictures, drawings and selections from the stories they had told.
nducting” at the center. The project was quite vague initially; it took shape slowly. Retrospectively, it consisted in eliciting stories and memories from residents during group sessions, using drawings and writings (draw a life tree, your first job, your first memory…). I also collected each resident’s narrative through repeated interviews or informal discussions during the day I spent at the center weekly. This resulted in individual booklets I made for each resident. These booklets contained pictures, drawings and selections from the stories they had told.
Each of these individuals represents a different way of engaging in the project, in various senses. This is what I want to reflect upon here.
An unfinished business
I will start with a short detour to stress the way this text extends and further explores some issues that I raised previously. In the course of my dissertation research, I formed the notion of social experience of mental illness to analyze long-term psychiatric care in France. I had been doing an ethnographic study, including interviews of patients and professionals, observations of various interactions between them in community mental health care centers and time spent with patients outside the center. What seemed particularly important to me was to avoid opposing an analysis of the psychiatric institution and of therapeutic practices to an analysis of the patient’s subjective experience. It was equally important that dealing with the illness’ embodied manifestations as well as with the mental health care providers were considered social processes interacting with others in the broader situation of the individual. Bridging different perspectives in medical anthropology, the notion of social experience allowed conceiving of mental illness as a dynamic process through which events, social constraints and resources come to constitute a life trajectory.
I was able to describe how people’s lives evolved in a dynamic process, where the affiliation to psychiatry and its importance in everyday life as a resource depended both on the availability of other resources (social, family…) and on the ability to maintain different social inscriptions in the face of disruptions (crisis, hospitalization) and of the manifestation of the illness.
As I sat in various group sessions, I examined how patients negotiated their “point of view”, or some sort of subjective view, with the care providers, emphasizing the fine line the actors walk, between the duty of the caretaker to protect and his/her goal of fostering autonomy.
In the whole research, the ways individuals recounted and conveyed this process were central methodological and epistemological concerns. Anthropologists have considered reflexively narrative and subjective experience, to emphasize that it is far from self-evident. Eliciting a life story or a narrative is necessarily a coproduction dependent on the context. Meeting individuals because of their belonging to psychiatry and of their having a diagnosis of mental illness frames the encounter, for example in terms of expectations that these issues are acknowledged or even accounted for in the narrative. Furthermore, a characteristic feature of mental illness is that the individual does not necessarily complies with the basic rules of interactions and of narrative, either because of delusions of or cognitive impairments. This gives the researcher even more reasons to reflect on the narrative’s coproduction.
I incorporated these concerns in the analysis of the social experience of mental illness. The repeated interviews I conducted allowed me to reconstitute multiple subject positions, as patient, as individual, as having a mental illness, as having to tell about their life and account for it. I attempted to bring together all these dimensions. It involved reflecting on the encounter of the researcher and the individual and on their engagement. The great importance of social expectations (whether one’s own, family or the interlocutor’s) in the way individuals shaped their stories constantly struck me.
Going back to the life story project, which was conducted independently from this research, I would like to focus on the dynamics between the engagement, of both the researcher and the individual, and the product of this encounter.
Coproducing an account of the past : defining the space of encounter and its product
I use the case of Carryl, Doris and John to reflect on the specific relationship each encounter produced, this relationship being the basis for the kind of narrative or production that we engaged in. I will describe successively each space of encounter and its attached narrative.
Reflecting on one’s past
 Carryl was tall and thin; he walked slowly, slightly bent, like an old man. He didn’t chat but he did engage in discussions. During our long taped interviews, he seemed to find with me a partner for real discussions, about culture and art, about history and philosophy. He also seized the opportunity of our interviews to talk about his life and turned it into a tool for introspection. From one meeting to another, he would go back to an event and try out a different analysis. In other words, the space of discourse Carryl and I shared was reflexive.
Carryl was tall and thin; he walked slowly, slightly bent, like an old man. He didn’t chat but he did engage in discussions. During our long taped interviews, he seemed to find with me a partner for real discussions, about culture and art, about history and philosophy. He also seized the opportunity of our interviews to talk about his life and turned it into a tool for introspection. From one meeting to another, he would go back to an event and try out a different analysis. In other words, the space of discourse Carryl and I shared was reflexive.
Carryl’s story started with his childhood in British Guyana. Although he was born in the US, his mother took him and his younger brother back to his grandparents after her divorce. Raised in a poor household, he nonetheless got the opportunity to go to high school because of his good grades and of his grandfathers’ pressure, but he had to stop and work at age 16. His mother kept her clerical job in Seattle and he didn’t see her again until he joined her at age 18. Remembering vividly his arrival to the US, he commented on his discovery of the contrast between what he called the aggressive way of US African-American/blacks, and his own passive attitude toward life. He related this attitude to the way black people were in Guyana, submitted to the British and the Queen and knowing their place. His narrative continued with the short time he spent in the army, not in combat, which offered him an opportunity to study psychology at the university, through the GI Bill. The story of his two short-lived marriages and of his moving from the West Coast to the East Coast were intertwined with his growing estrangement from life, which is how he described his illness, as with the various hospitalizations that ensued.
One of Carryl’s recurring interrogations in his account of his past was to wonder whether and how his life could have been different, without the illness. It is  interlaced with a “typical” severe mental illness narrative of the progressive loss of his social inscriptions and the subsequent adjustments: his wife divorcing him as he was hospitalized because “she had to go on with her life”, him having to quit his job and his mother then helping him find supported employment…
interlaced with a “typical” severe mental illness narrative of the progressive loss of his social inscriptions and the subsequent adjustments: his wife divorcing him as he was hospitalized because “she had to go on with her life”, him having to quit his job and his mother then helping him find supported employment…
As typical is his progressive integration into a supported mode of living, from the 30 years long janitor position he had at the hospital to the assisted housing and the 10 cigarettes and one dollar a day regime he complied to, commenting that he had become too dependent to live on his own.
Another question he asks is why the illness, why did it happen to him. As he recounts his life, he raises several hypotheses, such as the fact that his grandparents raised him, or that his mother left him when he was very young and that he grew up without seeing her, only reading her frequent letters, or else his “weakness” of character in an aggressive country, among other reasons.
In Carryl’s questions appear the intricate influences of illness and life opportunities in accounting for his current situation. At various points in his life, his expectations were deflected; they had to be reevaluated according to what was the range of the possible (when he went to high school but had to stop in order to work; when he came to the US, started working there, living with his wife; when he went to the university). This leads him to present himself as satisfied today although he underscores that is now dependent with no hope of this ever changing.
Fighting for survival

Carryl didn’t really get along with Doris, who was a character in the center. She spoke too loudly for him and was endlessly opinionated. She also appeared limited, which was reinforced by her childish manners. Our formal interviews were short; she seemed to be uncomfortable with them, maybe because she had few and scattered memories to put in the face of my questions. Many of her memories were so blurred that they seemed to melt. What we did was have long chitchatting sessions, where she would comment at length on given episodes of her life, telling a story of hardships, fights and survival. When we discussed, Doris called me “honey” every other sentence. She treated me as a granddaughter, using her life story both to give me an idea of how things were in her time and to give me sound advice. Our unspoken arrangement was about transmission. Her story is infused with energy to live and fight; it lacks reflexivity.
The story begins in 1929 in Mount Carmel, Illinois, where Doris grew up in a large family and with a mother who didn’t want her, who told her so and treated her different from the others since birth. Although Doris never understood her mother’s stance toward her, she did live, despite it. After Doris starts working, quite young, her story “goes West” when she decides she wants to see something else and goes to work there. A few years later she comes back to Illinois, because she misses her family. She expects things to have changed but finds herself admitted in the asylum by that very family instead. She seems to stay in Illinois for a while, first during a couple of years in the asylum and then in a group home where she is so miserable that she plans her flight. She goes East this time, to Washington, DC, where she doesn’t know anyone but finally settles, through a stay at the big St Elizabeth’s psychiatric hospital. She insists that people were nice to her in DC, and that in the asylum they “saved her”.
What she meant is that psychiatrists supported and helped her when her family and others let her down. After her escape, she had been through some great hardships and found valuable support in Washington’s psychiatric hospital, which she was grateful for and which helped her make it. Yet there was no mental illness in her story. The reason for her being in the asylum was the result of complex family dynamics. When she described her actions, feelings and situation, she was herself, the same herself that was speaking to me. This is very common in narratives of persons who have been psychiatric patients. However we want to characterize it (denial, memory loss, stigmatization…), the absence of mental illness and the presence of some life feature and experiences associated with it creates a void, something unspoken in our encounter.
From being the devil to talking about Jesus
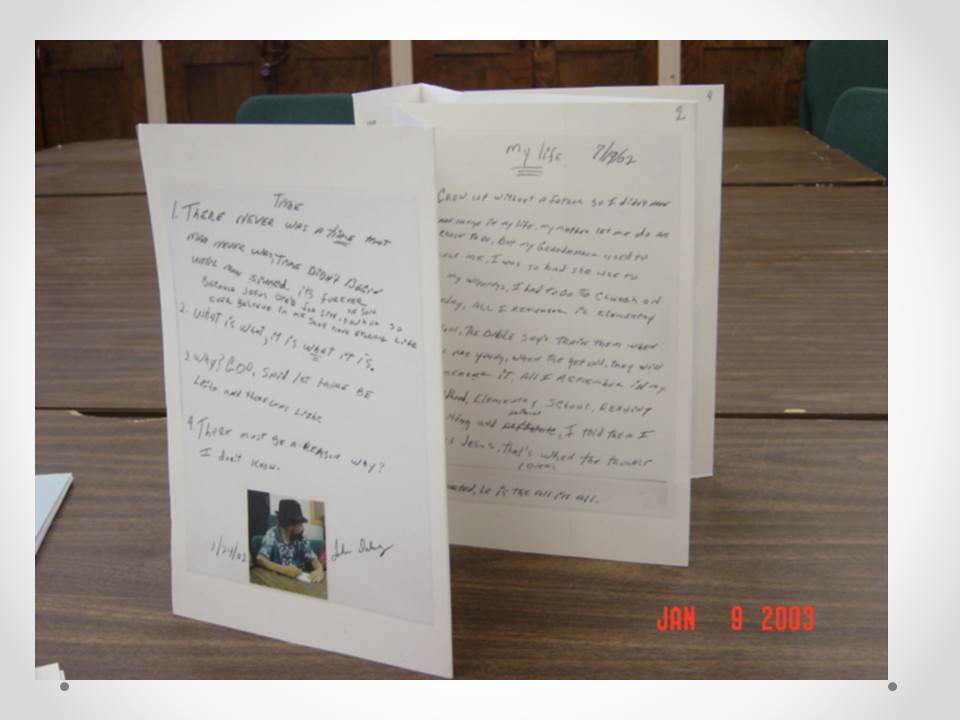
 Central to my relationship with John were his writings. During the art sessions, whatever the topic or task was, he would invariably spend his time writing on large white sheets of paper. In total, he wrote more than 50 small pieces, often with a title such as “my life” or “when I was young” but also “time” or “why”.
Central to my relationship with John were his writings. During the art sessions, whatever the topic or task was, he would invariably spend his time writing on large white sheets of paper. In total, he wrote more than 50 small pieces, often with a title such as “my life” or “when I was young” but also “time” or “why”.
These pieces would tell about events and moments in his life as well as evoke God and Jesus. They were repetitive, yet all different. A few times, I was able to draw him into more formal interviews. He answered my questions and inquiries without ever giving up his main task of delivering the word of God.
John’s narrative is less developed than the other two, yet is it also quite coherent and can be told as a story. This quote is the first piece John wrote when we started the project. More or less, it delineates the four periods John keeps referring to in all his writings. The first is when he was “Growing up”; he was cutting school and Church and smoking, although he notes that his grandmother, who raised him, did teach him “the right from the wrong”. The second period is when he was in the Navy; there he saw the world but most of all he kept “being the devil”, both drinking and gambling. His appreciation of that second period might be more ambiguous, though. At one point he explains how he “learned to be himself” when he was gambling. After his release from the Navy, due to an ear injury that leaves him partially deaf, then comes a time when John lives with various members of his family, working menial jobs and getting caught for a robbery which takes him in jail. The fourth period he describes starts with his admission to St Elizabeth’s hospital, in DC. He is admitted because no one outside wants to listen to him when he talks about being God and using God’s words. Thus, he appreciates being able to preach in the hospital, where, he says, “I thought good of myself, I thought Jesus, God and me. I still think so”, adding that “the patients would listen in the hospital. The psychiatrists wouldn’t listen, I had to teach them”.
John’ story intertwines elements from his familial and social life and events with the history of his relationship with God, which he also presents as a quest to know who he is. His is a story of redemption, since he went from being the devil to acting like Jesus. Yet when he refers to his current God-like attitude, he is sometimes explicitly using it metaphorically, other times literally, thus maintaining an ambiguity.
From the story to the social experience of mental illness
To conclude, what is to be found in these reconstituted narratives?
A medical anthropologist might find in these narratives exemplified features of the social experience of mental illness. In the way Carryl look for its possible causes and meaning; in the way Doris never acknowledges it in her experience, although she abundantly describes the asylums she was admitted to; in the way John subtly uses his delusional thoughts as a resource to define himself and his position.
The same medical anthropologist could be interested in how, at the end of one’s life, the signs of the illness and the contact with psychiatric care settings are leveled with other events in the life course, especially in a context of overall poverty. He might be struck by the fact that psychiatry, and especially the asylum, constitutes a resource for social support, such as housing and employment, in several life stories. All in all, these stories allude as much to the ways of dealing with the illness and with psychiatric care, as to the interweaving of historical events and social contexts with individual lives.
These narratives evoke labor migration between the US and (a British colony in) the Caribbean in the 1930’s; the self-consciousness of Carryl’s blackness and its differences with the African Americanness in the US of the 1950’s; Doris’ young adult life talks about being white in rural, poor country towns, living in old-style asylums; she also is one case of the large migration from southern states to Washington, DC that occurred in the middle of the century… There would be much more things. Among the others residents I met, a lot of them were black women and their work and family stories gave a vivid account of gender and racial segregation in pre- and post- civil rights’ Washington.
An anthropologist could be sensitive to the importance of taking into account the encounter in order to grasp the subject position these individuals adopt. There is a general frame to this encounter: they are all older people, well over 60, stabilized in a supported way of life (housing, activities) and not expected, because of their age, to display a personal project. In that sense, they are “beyond care” in the part that involves projects and social rehabilitation. Mental health care consists in meds and regular psychiatrist’s appointments. So, they have to find a way, a stance, to tell about their past with the weight of their current situation (and of how it accounts for it). Another element of the general frame is my approach to the project, the fact that I didn’t have an agenda as a researcher, and that they were quite free to seize my proposition or not, and to adapt its terms. In this context, to summarize the way these three individuals stage and plot their narrative, one could say that Carryl’s story is told as a reflection on his past life, oriented toward understanding how he ended up where he is now. Doris’ story is a narrative full of energy and fight and is structured around successfully overcoming hardships. John’s story tells about his redemption and his current missionary stance in life.
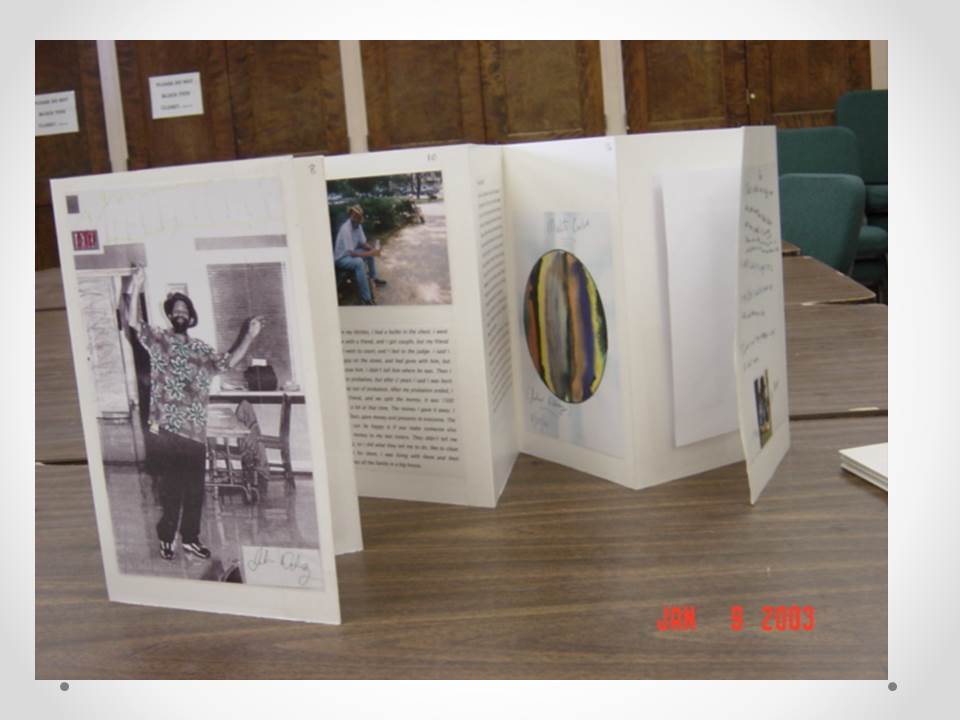
A random reader, though, might find that what happened during this project is not satisfyingly (or incompletely) conveyed in these reconstituted and commented on narratives. It might be necessary to pair them with another product of this project, which I would like to come back to as a conclusion. At the end of the year, I gathered all sorts of material attached to each of the persons who engaged in the project. There were drawings from the art sessions, writings from the writing sessions, pictures, either personal or taken during special activities at the center. I also chose parts from the interview transcripts, so as to convey best their style and mode of narration. I then selected and organized these materials, then pasted them on light cardboard. I gave each resident his or her booklet before I left. These were the traces of our encounter and engagement, something I made out of our material, for them.

John’s booklet